
Introduction
Hepatic encephalopathy (HE) is the most prominent neurocognitive complication of cirrhosis, represented by various manifestations of neuropsychiatric dysfunction that can be restrictive for patients’ lives and their caregivers, leading to increased mortality.[1] HE is clinically characterized by a disbalance in the sleep-wake cycle, which occurs with a shift from day to night and daytime sleepiness, confusion regarding both time and space, agitation or stupor, mental confusion, and even coma.[2]
The pathogenesis of HE is not yet fully elucidated, although it is recognized that ammonia accumulation, inflammation, oxidative stress, endothelial damage, and circulatory dysfunction collectively contribute significantly.[3,4] The mediators of inflammation act by modulating the cerebral effects of ammonia in cirrhosis. Furthermore, the reduction in serum albumin concentration, due to hepatic insufficiency, results in an increase in free metabolite levels, as the blood protein’s binding capacity is diminished, contributing to the precipitation of HE. The clinical neurological manifestations are associated with a sustained inflammatory response and endothelial disruption that is not suppressed by the current standard of care.[5]
In previous studies, the role of albumin has already been demonstrated for other complications of liver disease, such as in the control of ascites, spontaneous peritonitis, and hepatorenal syndrome, resulting in reduced hospitalizations and improvement in survival.[6,7] The objective of the present systematic review and meta-analysis is to evaluate the role of albumin in the management of HE.
Materials and Methods
Protocol and Registration
The systematic review and meta-analysis were conducted and structured in accordance with the Cochrane Handbook for Systematic Reviews of Interventions[8] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)[9] recommendations (Appendix Methods 1 and 2). The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO)[10] under the identification number CRD 42024545137.
Ethics Approval and Consent to Participate
This study is a systematic review and meta-analysis of previously published data and did not involve direct research with human participants, animals, or any individual-level data requiring ethical approval. All procedures of the included studies were conducted in accordance with the Declaration of Helsinki.
Consent for Publication
This manuscript does not contain any individual person’s data in any form; therefore, consent for publication was not required.
Eligibility Criteria and Outcomes
Inclusion in this meta-analysis was limited to studies that met all the following eligibility criteria: (i) randomized controlled trials (RCTs); (ii) enrolling patients with HE; (iii) comparing albumin to placebo; and (iv) reporting at least one of the outcomes of interest. There were no language or date restrictions. Abstracts, case reports, case series, editorials, letters to the editor, reviews, systematic reviews, and meta-analyses were excluded. The inclusion and exclusion criteria of each study are presented in Appendix Table 1.
The primary outcomes were mortality and clinical improvement in HE. Secondary outcomes were: (i) ammonia levels; (ii) liver transplantation; and (iii) significant adverse events (AE) rate. A subgroup analysis was performed in three studies to explore the impact of baseline HE severity by comparing outcomes between overt HE (oHE) and minimal HE (mHE) populations for the outcomes of HE improvement and ammonia levels.
Search Strategy and Study Selection
A systematic review of PubMed, Embase, and Cochrane Library databases was conducted on April 4, 2024. The search strategy was as follows: (albumin) AND (“hepatic encephalopathy”) AND (“randomized controlled trial”[pt] OR “controlled clinical trial”[pt] OR randomized [tiab] OR placebo[tiab] OR “drug therapy”[sh] OR randomly [tiab] OR trial[tiab] OR groups[tiab]). The search strategy was adapted to the different databases according to support for special characters. References of eligible papers, previous systematic reviews, and meta-analyses were also searched for additional studies of interest.
Two reviewers (AC and TC) conducted the search, imported results into Rayyan software,[11] and triaged the studies. After excluding duplicates and titles/abstracts clearly unrelated to the clinical question, the eligibility of each remaining study was assessed based on a full-text review of the articles. In instances of disagreement, a third reviewer (MF) was consulted.
Data Extraction
The following data were extracted from individual studies: (i) study characteristics, including the first author, year of publication, country of origin, sample size, and duration of follow-up; (ii) patient characteristics, including the number of patients, age, and gender; and (iii) outcomes, including improvement in encephalopathy, mortality, ammonia levels, liver transplantation, and AE rates. If the included studies did not provide mean and standard deviation, their values were estimated using the reported median and range, based on the methods described by Luo et al.[12–14] and Wan et al.[15]
Statistical Analysis
Statistical analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria) version 4.3.1. The Restricted Maximum Likelihood random effects model was employed for data synthesis. Treatment effects for dichotomous endpoints were compared using the Odds Ratio (OR) with corresponding 95% confidence intervals (CI), while continuous outcomes were assessed using the Mean Difference (MD). Statistical significance was defined as a p-value < 0.05. Heterogeneity was evaluated through I2 statistics and Cochran’s Q test. Significance for heterogeneity was determined as p<0.10 and I2>40%. In cases where significant heterogeneity was observed (I2>40%), sensitivity analyses were conducted to ensure the robustness and reliability of the findings. Forest plots were sorted by mean HE levels to help readers consider this variable when interpreting the results.
Trial Sequential Analysis
Trial sequential analysis (TSA) was performed using TSA software (Copenhagen Trial Unit, Centre for Clinical Intervention Research, Copenhagen)[16,17]. The effect measure (OD) was used, and a random effects model using the DerSimonian–Laird method was selected. No continuity correction was applied in the case of a zero event. The required sample size was estimated based on the calculated effect size for the intervention, considering a type I error of 5% and a power of 90%; benefit, harm, and inner wedge boundaries were drawn using the O’Brien–Fleming spending function. Heterogeneity correction was performed using model variance.
Risk of Bias and Evidence Quality Assessment
Two independent authors conducted the risk of bias assessment (AC and NM). Risk of bias in selected RCTs was assessed using the second version of the Cochrane Risk of Bias assessment tool (RoB 2)[18], evaluating five domains for each outcome of the selected studies: (i) bias in the randomization process; (ii) bias due to deviations from intended interventions; (iii) bias due to missing data; (iv) bias in outcome measurement; and (v) bias in the selection of the reported results.
The overall risk of bias assessment for each specific trial outcome was derived from individual domain judgments. Disagreements were resolved through consensus after discussing the reasons for the discrepancy.
Results
Study Selection and Baseline Characteristics
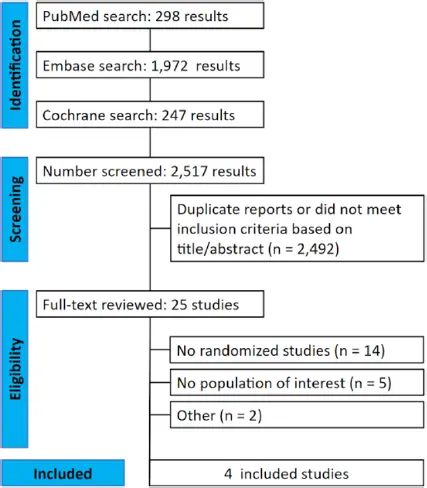
As detailed in Figure 1, the initial search yielded 2,517 results. After the removal of duplicate records and ineligible studies, 25 remained and were fully reviewed. Of these, a total of 4 studies [19–22] were included (306 patients, with albumin administered to 150 and placebo to 156 patients). Baseline characteristics were described in Table 1, and the principal characteristics of the studies were reported in Table 2. Other characteristics were described in Appendix Table 2.
| Study | Follow-up (days) | Treatment | Sample size | Age (years) | Male sex | Etiology of cirrhosis | MELD-Na score | Serum albumin | previous HE | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HCV | HBV | Alcohol | NAH | Others | |||||||||
| Fagan et al.[19] | 35 | 25% IV albumin (1.5 g/kg body weight) | 24 | 63.83±6.99 | 22 (92) | 3 | – | 12 | 7 | 2 | 11.75±3.78 | 3.38±0.36 | – |
| Placebo | 24 | 62.21±8.59 | 21 (88) | 4 | – | 10 | 10 | 0 | 10.46±3.36 | 3.20±0.38 | – | ||
| Sharma et al.[22] | 10 | Albumin 1.5 gm/kg/day + control | 60 | 42.5±8.7 | 49 | 5 (8.3) | 12 (20) | 35 (58.3) | – | 8 (13.3) | 26.4±5.8 | 2.3±0.9 | 27 (45) |
| lactulose 30–60 ml three times a day | 60 | 38.4±9.6 | 51 | 6 (10) | 13 (21.6) | 32 (53.3) | – | 9 (15.0) | 25.8±5.1 | 2.4±0.8 | 24 (40) | ||
| Simón-Talero et al.[21] | 90 | 20% IV albumin (1.5 g/kg body weight) | 26 | 63.7±11.3 | 19 (73.1) | 9 (34.6)† | 7 (26.9) | – | 6 (23.1) | 16.8±3.8 | 2.9±0.6 | – | |
| Placebo | 30 | 66.3±9.7 | 23 (76.7) | 10 (33.3)† | 17 (56.7) | – | 2 (6.7) | 16.1±5.1 | 3.0±0.6 | – | |||
| Ventura-Cots et al.[20] | 180 | IV albumin (1.5 g/kg body weight) | 40 | 66.5 (59.9–73.6)* | 29 (72.5) | 6 (15) | – | 19 (47.5) | – | 9 | 17 (15–20)* | 2.6 (2.41–2.93)* | 26 (65) |
| Placebo | 42 | 69.1 (63.3–75.3)* | 26 (61.9) | 4 (9.5) | – | 22 (52.3) | – | 9 | 17 (16–20)* | 2.85 (2.35–3.01)* | 27 (64.3) |
| Author, year | Follow-up (days) | Location; Period | Center | N | Treatment | Results (I x C) |
|---|---|---|---|---|---|---|
| Sharma et al.[22] | 10 | India; 2015–2016 | Multicentric | 120 | I: lactulose + albumin C: lactulose |
HE recovery: 75% x 53.3% (p=0.03) Hospital stay: 6.4±3.4 days x 8.6±4.3 days (p=0.01) Mortality: 18.3%x31.6% (p=0.04) Arterial ammonia (µmol/L): 78.1±14.8 (p<0.001) x 78.9±15.2 (p=0.001) TNF alfa (pg/mL): 21.8±8.9 (p=0.001) x 30.6±9.8 (p=0.02) IL-6 (pg/mL): 18.1±6.4 (p=0.01) x 24.3±7.3 (p=0.03) IL-18 (pg/mL): 41.9±10.4 (p<0.001) x 60.0±14.4 (p=0.04) Endotoxin (EU/mL): 0.25±0.08 (p<0.001) x 0.38±0.07 (p=0.01) |
| Fagan et al.[19] | 35 | USA; 2018–2022 | Unicenter | 48 | I: albumin C: placebo (saline) |
MHE frequency: 79% (p=0.05) x 96% (p=0.96) Venous ammonia: 64.81±41.1 (p=0.20) x 78.46±41.78 (p=0.42) IL-1b (pg/ml): 0.35±0.37 (p<0.05) x 0.47±0.50 IL-6 (pg/ml): 3.18±1.73 x 4.94±7.52 TNF alfa (pg/ml): 15.06±7.94 x 16.88±7.32 IL-10 (pg/ml): 3.28±1.81 x 3.08±3.02 (p<0.05) LBP (ng/ml): 1,659.7±931.6 x 1,931.2±316.7 ICAM-1 (ng/ml): 313.1±125.6 x 343.6±125.9 (p<0.05) ADMA (lM): 0.63±0.10 (p<0.05) x 0.65±0.14 IMA (IU/ml): 1 |
| Ventura-Cots et al.[20] | 180 | Spain; 2015–2019 | Multicentric | 82 | I: albumin C: placebo (saline) |
Transplant-free survival at 90 days: 91.9% x 80.5%(p=0.3) 90-day cumulative incidence of death: 9% x 20% (p=0.1) Transplant-free survival at 180 days: 79.7% x 67.8% (p=0.2) 180-day cumulative incidence of death: 11% x 28% (p=0.09) |
| Simón-Talero et al.[21] | 90 | Spain; 2009–2012 | Multicentric | 56 | I: albumin C: placebo (saline) |
Hospital stay: 7.0 (IQR 4.5–10.0) x 7.0 (IQR 4.8–11.0) (p=0.8) Transplant-free survival at 90 days: HR 0.37, CI 95% 0.16-0.89, p=0.02 Ammonia (µmol/L): 97 (IQR 59–134) x 113 (IQR 54–132) Renin (µIU/ml): 54.3 (IQR 14.0–226.9) x 138.2 (IQR 15.2–392.0) IL-6 (pg/ml): 275.6 (IQR 142.2–554.6) x 276.1 (IQR 157.1–642.2) IL-10 (pg/ml): 10.9 (IQR 7.2–17.2) x 13.8 (IQR 8.6–18.9) TNF (pg/ml): 45.4 (IQR 25.6–103.4) x 34.3 (IQR 26.0–68.9) MDA (nmol/ml): 2.4 (IQR 2.0–3.1) x 2.3 (IQR 2.1–3.4) sCD163 (ng/ml): 27.9 (IQR 23.7–29.6) x 24.4 (IQR 18.6–29.8) |
The administration of albumin versus placebo varied slightly across the included studies. Fagan et al.[19], Simón-Talero et al.[21], and Ventura-Cots et al.[20] all administered intravenous albumin at a dose of 1.5 g/kg body weight, using placebo as the comparator. In contrast, Sharma et al.[22] provided albumin at a dose of 1.5 g/kg/day in combination with standard lactulose therapy, while the control group received lactulose alone (Table 1).
Pooled Analysis of All Studies
Primary Outcome
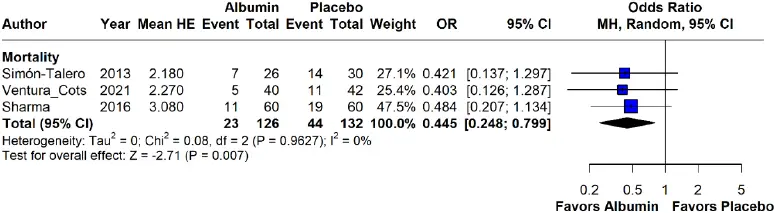
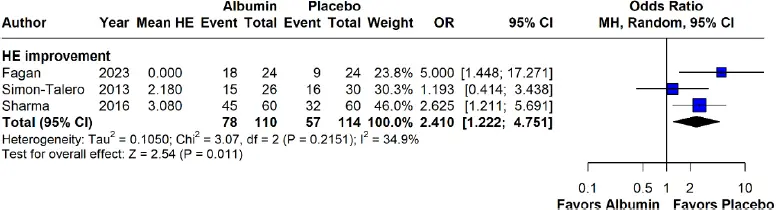
Mortality was reported in three studies (258 patients), and the analyses showed a significant difference favoring albumin use (OR 0.44; 95% CI 0.24 to 0.79; p=0.007; I2=0%; Fig. 2). The clinical improvement rate of HE was reported in three studies (224 patients), and the analyses also showed a significant difference favoring albumin use (OR 2.41; 95% CI 1.22 to 4.75, p=0.011; I2=34.9%; Fig. 3).
Secondary Outcomes
Three studies evaluated ammonia levels (219 patients), and there was no significant difference between groups (MD -1.46; 95% CI -6.62 to 3.71; p=0.58; I2=0%; Appendix Fig. 1). Two studies evaluated the evolution to liver transplantation (138 patients), and there was no significant difference between groups (OR 0.73; 95% CI 0.12 to 4.37; p=0.732; I2=35%; Appendix Fig. 2). Two studies evaluated the significant AE rate (202 patients), and there was also no difference between groups (OR 1.24; 95% CI 0.57 to 2.68; p=0.586; I2=0%; Appendix Fig. 3).
Subgroup Analysis
A subgroup analysis was performed in three studies to explore the impact of baseline HE severity by comparing outcomes between oHE and mHE populations. No statistically significant difference was observed between groups in HE improvement (OR 2.41; 95% CI 1.22 to 4.75; p=0.1982; I2=34.9%; Appendix Fig. 4) or ammonia levels (MD -1.46; 95% CI -6.62 to 3.71; p=0.2960; I2=0%; Appendix Fig. 5). Mean HE refers to the weighted average of baseline HE grades among patients included in each study.
Trial Sequential Analysis
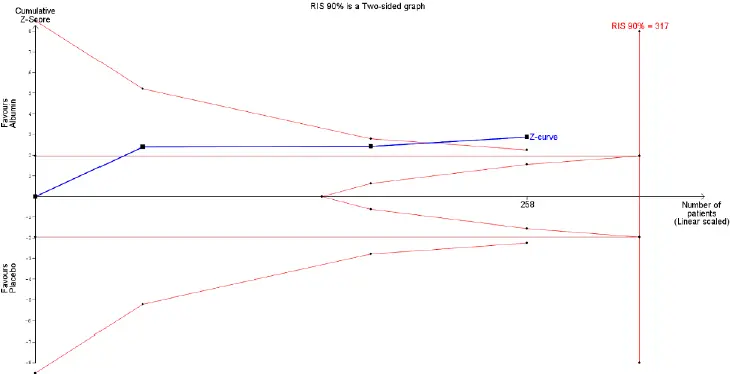
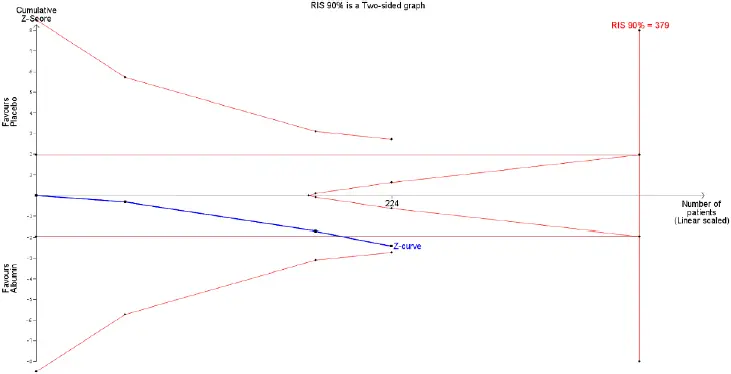
In the TSA for mortality, the cumulative z-line crossed the boundary for effect but did not reach the required sample size (Fig. 4). These findings suggest that, although the pooled effect is statistically significant, with regard to sample size, the result is not definitive, and future studies are necessary to be conclusive about the use of albumin to reduce mortality in this population.
In the TSA for HE improvement, the cumulative z-line lies in the zone with no statistical significance (Fig. 5). This finding implies that the sample size of the meta-analysis was too small, and it is therefore impossible to infer where the cumulative z-line will lie in future trials. No conclusions regarding the meta-analysis pooled effect for HE improvement can be made.
Risk of Bias and Evidence Quality Assessment
The studies of Simón-Talero et al.[21], Fagan et al.[19], and Ventura-Cots et al.[20] were at low risk of bias according to the RoB 2 tool (18). However, the trial by Sharma et al.[22] was at moderate risk due to the lack of blinding (Appendix Table 3).
Discussion
The results of this meta-analysis corroborated those reported in a previous one by Is et al.[23], with a statistically significant difference favoring albumin in HE improvement and reduced mortality. There were no differences in ammonia levels, evolution to liver transplantation, and AE rates of the treatment compared to the placebo group. This study has some advantages over previous meta-analyses on the topic.[23] Firstly, it included 2 new studies, Fagan et al.[19] and Ventura-Cots et al.[20], increasing the sample size by 73.8%, providing a more accurate result. Second, a TSA was performed to determine when the pooled effect is strong enough to be unlikely to be changed by more studies, helping to balance type I and II errors. Third, additional outcomes were evaluated, including serum ammonia levels, progression to liver transplantation, and AE rates.
Findings from the present meta-analysis are also in line with those reported by Bai et al.[24] in a single-center retrospective study and a meta-analysis that demonstrated albumin infusion may prevent the occurrence of oHE and improve its severity in patients with cirrhosis. A subsequent meta-analysis[25] including 42 RCTs further showed that human albumin treatment significantly improved the severity of complications in cirrhotic patients, including those with HE. Moreover, in 2023, an international position statement[26] supported the benefits of human albumin in reducing the incidence of HE, improving its severity, and lowering mortality in HE patients. However, the quality of available evidence was limited by heterogeneity in study design and subjectivity in outcome assessment. The current meta-analysis aims to address these limitations by providing greater clarity on these important findings.
The clinical and psychosocial burden of HE relies on the patients, the relatives, and the healthcare system.[27,28] In the US, there are no other FDA-approved therapies other than lactulose and rifaximin for this condition. (2) The idea in conducting this meta-analysis is based on the theory that HE can be caused by a sum of ammonia accumulation, inflammation, oxidative stress, and endothelial damage. In this context, it is hypothesized that albumin can act as a mediator of the inflammatory response and endothelial dysfunction in HE.[22,29]
HE refers to the broad spectrum of neuropsychiatric disturbances associated with acute or chronic liver failure, as well as portosystemic shunting, in the absence of underlying hepatocellular disease. The pathophysiology of HE remains incompletely elucidated but is recognized as multifactorial. Nevertheless, hyperammonemia is a well-documented contributor to its development. This condition results from hepatic dysfunction and the consequent impairment of ammonia metabolism, leading to its accumulation in the bloodstream. The excess ammonia is absorbed by astrocytes in the brain, where it is converted into glutamine, leading to osmotic stress, astrocyte swelling, and subsequent brain dysfunction.[30] Despite its significant role in the development of HE, discrepancies exist in the literature regarding the direct correlation between ammonia levels and the severity of HE in patients with cirrhosis. This has contributed to the general consensus that hyperammonemia is unlikely to be the only determinant of the neurocognitive sequelae, with other contributing factors involved.
Current treatments for oHE are focused on reducing ammonia production and/or enhancing its elimination, as well as promptly correcting precipitating factors. However, there are no interventions specifically targeting the other contributing factors.[31] In this context, albumin becomes a particularly interesting option due to its effects in modulating systemic inflammation. It is known that albumin has antioxidant effects, due to its ability to bind free metals and capture free radicals, and bilirubin bound to albumin inhibits lipid peroxidation, representing an indirect antioxidant effect.[29]
Additionally, a notable characteristic of albumin is its ability to bind to pro-inflammatory substances and mediators of inflammation, thereby attenuating endothelial dysfunction and vasodilation.[22] Furthermore, systemic inflammation not only leads to circulatory dysfunction, which reduces cerebral perfusion[32], but also enhances the inhibitory effect of ammonia on brain function.[5] Therefore, considering the potential impact of systemic inflammation on the decompensation of cirrhosis in the presence of HE, as well as albumin’s role in modulating innate immune responses and oxidative stress, it is plausible to propose that some of albumin’s effects may be related to these underlying mechanisms.
This meta-analysis found no significant differences in ammonia levels or liver transplantation rates, challenging the mechanistic rationale for albumin’s benefits linked to hyperammonemia pathophysiology. Furthermore, in the study by Fagan et al.[19], there was no significant change in liver disease severity or venous ammonia levels between or within groups; however, improvements were observed in systemic inflammation and endothelial dysfunction. This may account for the greater improvement in the Portosystemic Hepatic Encephalopathy Scores (PHES), which are associated with inflammation, as opposed to critical flicker frequency (CFF), a neurophysiological test that may be more closely linked to ammonia levels.[19] Simón-Talero et al.[21] investigated oHE and found no correlation between increased survival and inflammatory markers or ammonia levels, leaving an unresolved question regarding the mechanism by which albumin might reduce mortality.[21] Sharma et al.[22] examined the combined use of lactulose and albumin in oHE patients and observed a greater reduction in inflammatory markers (such as cytokines), although ammonia levels decreased equally in both treatment groups. In contrast, Ventura et al.[20] studied oHE and was unable to demonstrate a reduction in mortality and did not assess systemic inflammation.
Some non-randomized studies also reported similar results. Jalan et al.[4] evaluated patients with HE receiving albumin or not and demonstrated that the severity of HE was significantly improved in the albumin group. The single-center retrospective study by Bai et al.[24] demonstrated that albumin infusion was linked to a decreased incidence and improvement of oHE, potentially correlating with reduced in-hospital mortality among cirrhotic patients, regardless of oHE status. Furthermore, long-term albumin administration demonstrated prolonged overall survival and acted as a disease-modifying treatment for HE in the open-label RCT by Caraceni et al.[7] Additionally, it improved survival and reduced emergent hospitalizations in the non-randomized prospective study conducted by Di Pascoli et al.[6]
In terms of severity, HE is classified as covert or mHE, characterized by minor or no symptoms but with abnormalities on neuropsychological and/or neurophysiological tests, or oHE, which is defined as grades II or higher according to the West Haven criteria.[33] This study included three studies focused on populations with oHE, while one study involved patients with mHE and a prior oHE event classified as grade zero. This characteristic was detailed in Table 3, which highlights the heterogeneity in patient populations across the included studies, with varying distributions of baseline HE grades and differing proportions of patients with previous HE episodes. This variability may introduce bias and influence the interpretation of outcomes.
Despite this study having a population predominantly based on oHE, mHE has been described as a condition present in up to 80% of individuals with stable cirrhosis, which predisposes them to the development of oHE.[34,35] Even after maximal treatment of symptoms of HE, most patients had not fully restored their cognitive function and remained with mHE, which is defined as a condition where patients with cirrhosis have a normal neurological examination but exhibit measurable cognitive impairments.[19] The diagnosis of mHE is currently based on abnormalities in neurophysiological, neuropsychological, or psychophysical tests.[2] It is already recognized that this subset of patients has an increase in mortality due to future HE.[35] The study by Fagan et al.[19] showed that albumin promotes the reversal of mHE, which can be another clinical benefit of albumin use in patients in this context.
| Autor, year | Clinical characteristics | Baseline HE grade 0/1/2/3/4* | Previous HE episodes n (%) |
|---|---|---|---|
| Sharma et al.[22] | Overt HE | 0/0/27/57/36 | 51 (42.5) |
| Fagan et al.[19] | mHE with prior overt HE** episode | 48/0/0/0/0 | 48 (100) |
| Ventura-Cots et al.[20] | Overt HE*** | 0/0/61/20/1 | 53 (64.6) |
| Simón-Talero et al.[21] 2013 | Overt HE*** | 0/0/46****/10 | 36 (64.2) |
Limitations
The study has limitations. First, there are only four RCTs evaluating the use of albumin in the HE population, with a pooled small sample size, which may compromise the reliability of the results. A TSA was conducted to estimate the required sample size while balancing type I error. This analysis indicated that the required sample size was not achieved, highlighting the need for future multicenter trials with larger cohorts to validate the reduction in mortality and improve statistical power. Second, one of the studies was not blinded, increasing the risk of publication bias and potentially affecting the generalizability of the findings. Finally, the populations of the included studies vary in terms of HE severity, as shown in Table 3. This variability may have influenced the results, underscoring the importance of evaluating each subgroup to determine the true effect of the treatment in specific populations.
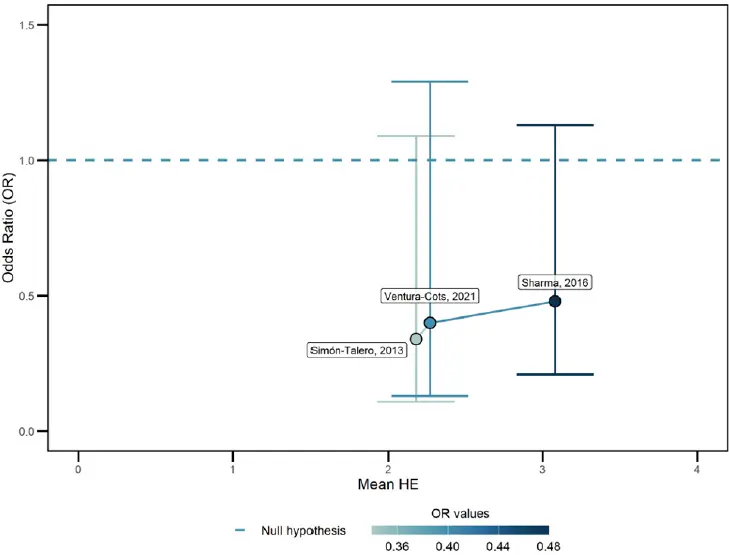
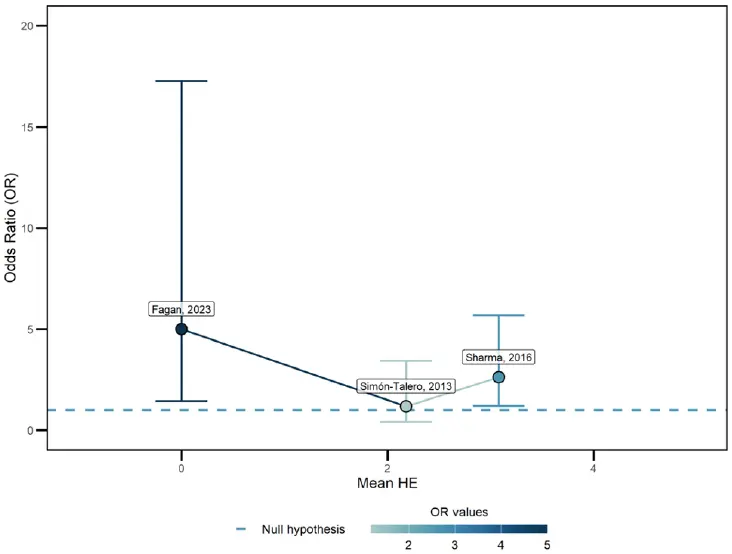
Scatter plots (Fig. 6, 7, and Appendix Fig. 6–8) were employed to assess the impact of baseline HE on the respective outcomes: mortality, HE improvement, ammonia levels, liver transplantation, and AEs. The analysis revealed no clear evidence that baseline HE significantly influenced these outcomes. The scatter plots highlighted the heterogeneity across the studies, and no definitive conclusions could be drawn. Furthermore, a subgroup analysis was performed for the two outcomes that included studies with both oHE and mHE populations: HE improvement and ammonia levels, neither of which showed statistical significance (Appendix Fig. 4, 5). Further research with larger sample sizes and standardized methodologies is essential to better understand the effect of baseline HE on patient outcomes.
However, our study also has strengths, such as the inclusion of only RCTs, which reduces the bias of selection, and the TSA, which helps to balance type I and II errors and determines when the pooled effect is strong enough to be unlikely to be changed by more studies.
Conclusion
This meta-analysis showed that albumin infusion should be considered in the treatment of HE, as its use resulted in better clinical improvement and lower mortality rates. However, as indicated by the TSA, new RCTs with larger sample sizes, multi-center designs, and greater diversity in patient populations are necessary to reach a definitive conclusion on this topic. Future studies should aim to identify the specific HE populations that would benefit the most from this treatment, delineating subgroups for oHE and mHE, as well as addressing specific patient comorbidities.
Online Appendix Link
https://hepatologyforum.org/storage/upload/files/1761307426-appendix-en.pdf
Ethics Committee Approval
Not applicable. This study did not involve human participants, animal subjects, or any data requiring ethical approval.
Conflict of Interest
All authors report no relationships that could be construed as a conflict of interest. and take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Financial Disclosure
Not applicable. This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Use of AI for Writing Assistance
All data generated or analysed during this study are included in this published article [and its supplementary information files]. The authors confirm that no artificial intelligence (AI)–assisted technologies, such as Large Language Models (LLMs), chatbots, or image creators, were used in the production of this work.
Author Contributions
Concept – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF; Design – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF; Supervision – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF; Data Collection and/or Processing – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF; Analysis and/or Interpretation – ACC, VALJ, AAP, TLC, MVF; Literature Review – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF; Writing – ACC, MVF; Critical Review – ACC, VALJ, AAP, NJM, TLC, OCM, PR, ESBJ, AMR, MVF.
Peer-review
Externally peer-reviewed.
How to cite this article: Covre Coan AC, Antunes VLJ, Prata AA, Milioli NJ, Correa TL, Cosendey O, Romeiro P, et al. Use of albumin in patients with hepatic encephalopathy: A systematic review and meta-analysis of randomized controlled studies with trial sequential analysis. Hepatology Forum 2026; 7(1):4–13.
References
- Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology 2009
- Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J Hepatol 2014
- Hepatic Encephalopathy. StatPearls 2025
- Reversal of diuretic-induced hepatic encephalopathy with infusion of albumin but not colloid. Clin Sci (Lond) 2004
- Role of ammonia and inflammation in minimal hepatic encephalopathy. Metab Brain Dis 2007
- Long-term administration of human albumin improves survival in patients with cirrhosis and refractory ascites. Liver Int 2019
- Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial. Lancet 2018
- Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane 2023
- The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021
- . 2019
- AI and the evolution of journalistic practices. J Inform Stud Technol 2025
- Detecting the skewness of data from the five-number summary and its application in meta-analysis. Stat Methods Med Res 2023
- Optimally estimating the sample standard deviation from the five-number summary. Res Synth Methods 2020
- Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res 2018
- Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014
- Interpreting trial sequential analysis. Transfusion 2016
- Explanation of trial sequential analysis: using a post-hoc analysis of meta-analyses published in Korean Journal of Anesthesiology. Korean J Anesthesiol 2021
- RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019
- A double-blind randomized placebo-controlled trial of albumin in outpatients with hepatic encephalopathy: HEAL study. J Hepatol 2023
- Effects of albumin on survival after a hepatic encephalopathy episode: Randomized double-blind trial and meta-analysis. J Clin Med 2021
- Effects of intravenous albumin in patients with cirrhosis and episodic hepatic encephalopathy: a randomized double-blind study. J Hepatol 2013
- Randomized controlled trial comparing lactulose plus albumin versus lactulose alone for treatment of hepatic encephalopathy. J Gastroenterol Hepatol 2017
- Albumin in the management of hepatic encephalopathy: A systematic review and meta-analysis. Ann Hepatol 2021
- Albumin infusion may decrease the incidence and severity of overt hepatic encephalopathy in liver cirrhosis. Aging (Albany NY) 2019
- Use of human albumin infusion in cirrhotic patients: a systematic review and meta-analysis of randomized controlled trials. Hepatol Int 2022
- Use of albumin infusion for cirrhosis-related complications: An international position statement. JHEP Rep 2023
- Financial burden in adults with chronic liver disease: A scoping review. Liver Transpl 2022
- Cognitive dysfunction is associated with poor socioeconomic status in patients with cirrhosis: an international multicenter study. Clin Gastroenterol Hepatol 2013
- Human serum albumin, systemic inflammation, and cirrhosis. J Hepatol 2014
- Pathogenesis of hepatic encephalopathy: role of ammonia and systemic inflammation. J Clin Exp Hepatol 2015
- Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014
- Increased cerebrovascular resistance in cirrhotic patients with ascites. Hepatology 1998
- Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna 1998. Hepatology 2002
- Subclinical hepatic encephalopathy predicts the development of overt hepatic encephalopathy. Am J Gastroenterol 2001
- Predicting overt hepatic encephalopathy for the population with cirrhosis. Hepatology 2019

